


This comparison matters more than it might seem, because the single most frustrating experience in pigment treatment is applying the right expectations to the wrong type. If you are treating melasma and expecting it to behave like PIH, you will feel like you are failing when you are not. If you are treating PIH and managing it like melasma, you may be overcomplicating something that would have resolved on its own.
The two types look similar on the surface. But underneath, they are completely different animals.
The fundamental difference
PIH is a mark left by a past event. Something inflamed the skin (a breakout, a burn, an irritation, a procedure), the inflammation triggered excess melanin production in that area, and the event resolved. The pigment remains, but the cause is over. The body is already in the process of clearing it. The trajectory is forward.
Melasma is a pattern driven by present and future triggers. The melanocytes in the affected area are being influenced by ongoing inputs: hormonal fluctuations, UV exposure, heat, and sometimes internal factors. The cause is not a past event. It is a current condition. The trajectory is not straightforward because the triggers keep cycling.
That one difference changes everything about how the timeline behaves.
How PIH progresses
PIH follows a broadly linear path. Once the trigger resolves and the skin is protected, the pigment fades gradually as the skin turns over and pigmented cells are replaced by normally pigmented ones. The speed depends on depth, skin tone, and whether the trigger has truly stopped, but the direction is consistent. It gets better over time.
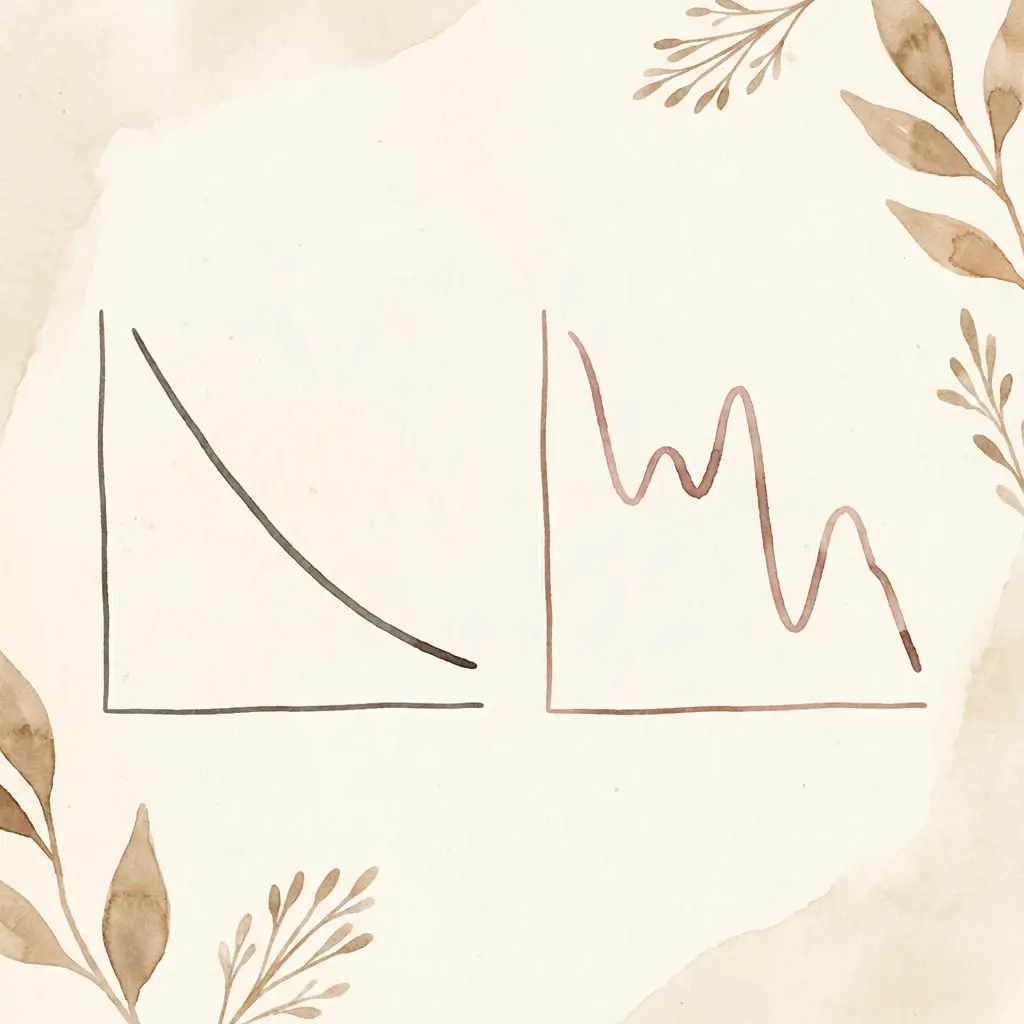
Typical PIH arc: Trigger resolves → inflammatory signalling winds down → cell turnover carries pigmented cells to the surface → mark lightens → mark resolves (weeks to months for epidermal, months to longer for dermal)
Progress is measurable. Comparison photos show steady improvement. Setbacks are unusual unless the trigger recurs or sun exposure re-darkens the area.
How melasma progresses
Melasma does not follow a linear path. It fades, it flares, it responds to seasonal changes, hormonal shifts, and stress in ways that are not always predictable. A good month does not guarantee the next month will be good. A flare does not mean the treatment has failed.
Typical melasma arc: Trigger ongoing → improvement with treatment and trigger control → flare with hormonal shift, sun, or heat → recovery → new baseline (potentially better than before) → repeat
Progress is measured in baselines over months, not in week-to-week comparisons. The trajectory is generally positive for people who manage it well, but it is not smooth. The peaks get lower, the recoveries get faster, and the overall pattern improves. But the pattern is a wave, not a line.
Why applying PIH expectations to melasma causes problems
If you expect melasma to behave like PIH, you expect steady, visible improvement over a defined timeline. When that does not happen, the natural conclusion is that the treatment is not working. So you switch products. Or you escalate to something stronger. Or you give up.
All three of those responses make melasma worse. Switching products too frequently never gives any single approach enough time to work (three months minimum for melasma). Escalating to stronger actives increases the risk of barrier damage and rebound inflammation. And giving up means abandoning an approach that may have been working but just had not cleared the minimum assessment window yet.
The fix is not trying harder. It is recalibrating what "working" looks like. For melasma, working means your baseline is better than it was six months ago. Working means flares recover faster. Working means the management strategy is sustainable and the trend is positive even through the fluctuations.
Quick comparison
| PIH | Melasma | |
|---|---|---|
| Trigger | Past event (breakout, burn, procedure) | Ongoing (hormones, UV, heat) |
| Trajectory | Generally linear improvement | Non-linear, fluctuating |
| Assessment window | 4 to 12 weeks | 3 to 6 months minimum |
| "Faded" means | Resolved or nearly resolved | Baseline improved, not necessarily resolved |
| Maintenance | Protect from recurrence | Ongoing management essential |
| Response to escalation | Sometimes helpful if matched to depth | Often counterproductive |
Why type identification matters so much
If you are not sure which type you are dealing with, every decision downstream is potentially mismatched. The treatment approach, the assessment window, the definition of success, and the long-term strategy all depend on getting the type right.
Some clues that can help. PIH usually appears as a defined mark in a location where a specific event happened. You can often remember the breakout, the irritation, or the injury that caused it. Melasma usually presents as a diffuse, symmetrical pattern across the cheeks, forehead, upper lip, or jawline, without a clear triggering event in that specific area.
But these patterns overlap, especially on melanin-rich skin where both types can appear dense and dark. If you are managing pigment that is not responding the way you expect, confirming the type with a dermatologist is one of the most efficient steps you can take.
PIH and melasma share a surface resemblance and almost nothing else. Matching your expectations to the right type is the difference between feeling like your approach is failing and understanding that it is working on a different timeline.


