


A breakout leaves a dark mark. A mosquito bite leaves a dark mark. Eczema clears up and leaves a shadow. Friction from a bra strap darkens the skin underneath. A laser treatment meant to fix pigmentation somehow makes it worse.
These feel like completely different problems. Different causes, different body parts, different circumstances. But they all end in the exact same place: pigment that was not there before, sitting stubbornly in your skin.
That is not a coincidence. That is a pattern.
And once you see the pattern, hyperpigmentation stops feeling so random and starts making a frustrating amount of sense.
So what is the pattern?
Almost every trigger that leads to hyperpigmentation runs through a single biological pathway: inflammation.
Not the dramatic kind. Not red, swollen, obviously-something-is-wrong inflammation. The kind behind most hyperpigmentation is quiet. Low-grade. Invisible. It operates beneath the surface, talking directly to the cells that produce pigment, telling them to ramp up.
This is why a sunburn and a hormonal shift and a post-acne mark can all produce the same result. On the surface, they look nothing alike. Underneath, they speak the same language: inflammatory signalling.
Most skincare content treats each trigger as its own separate problem with its own separate solution. UV damage gets one article. Acne marks get another. Hormonal pigmentation gets a third. But none of them explain why the end result is always the same.
That is the piece worth understanding. Because once you see what is happening underneath, you stop falling for approaches that sound right but actually make things worse. You start asking better questions. And you stop blaming yourself when a product that "works for everyone" does not work for you.

What inflammation actually does to your pigment cells
Quick biology. This is the part that makes everything else click.
Your skin contains specialised cells called melanocytes. Their job is to produce melanin, the pigment that gives your skin its colour and protects it from UV damage. Under normal conditions, they produce melanin at a steady, regulated rate. Your baseline skin tone is the result of that steady output.
Inflammation disrupts the regulation.
When skin tissue gets stressed, damaged, or irritated, your immune system sends out a flood of signalling molecules: prostaglandins, cytokines, leukotrienes, reactive oxygen species. These are the defence team. They rush to the problem, recruit immune cells, and kick off repairs.
Here is the catch: your melanocytes are listening to those same signals.
They sit right at the junction between your epidermis and dermis, surrounded by immune activity. When inflammatory messengers flood the area, melanocytes read it as a call to action. They ramp up an enzyme called tyrosinase (the rate-limiting step in melanin production), which means more melanin, which means darker pigment deposited into the surrounding skin cells.
This is actually a protective response. Melanin absorbs UV, neutralises free radicals, and shields your DNA. Your body makes more of it when it senses your skin is under threat. In evolutionary terms, this is brilliant engineering. Your skin detects danger and builds a stronger shield.
The problem is that the engineering has no off switch for "minor inconvenience."
The problem is twofold:
- The response does not always match the threat. A minor irritation can trigger a outsized pigment response, especially in skin that is already sensitised.
- The response does not always switch off. Melanocytes can stay in an activated state, overproducing melanin long after the original trigger is gone. They essentially get stuck in high gear.
One more layer. The melanin produced during an inflammatory episode gets packaged into structures called melanosomes, which transfer to surrounding skin cells. In lighter skin, melanosomes tend to be smaller and cluster together, making them easier for the body to break down during normal turnover. In darker skin, they are larger, more densely packed, and distributed individually throughout the cell. Same inflammatory event. But the mark lasts longer and shows more prominently.
Why the mark outlasts the thing that caused it
This is where it gets properly frustrating, and where most explanations stop short.
Acute inflammation is designed to be temporary. You cut your finger, the area swells, repair happens, inflammation resolves. Any pigment change during that process often fades naturally as the skin turns over and the signals quiet down.
But when inflammation is sustained, repeated, or triggered in skin that responds strongly, the pigment production does not resolve cleanly.
What happens instead:
- The cells stay ramped up, continuing to produce excess melanin
- The inflammatory environment can become self-sustaining (damaged tissue releases signals that recruit more immune activity, which causes more signalling, which keeps melanocytes activated)
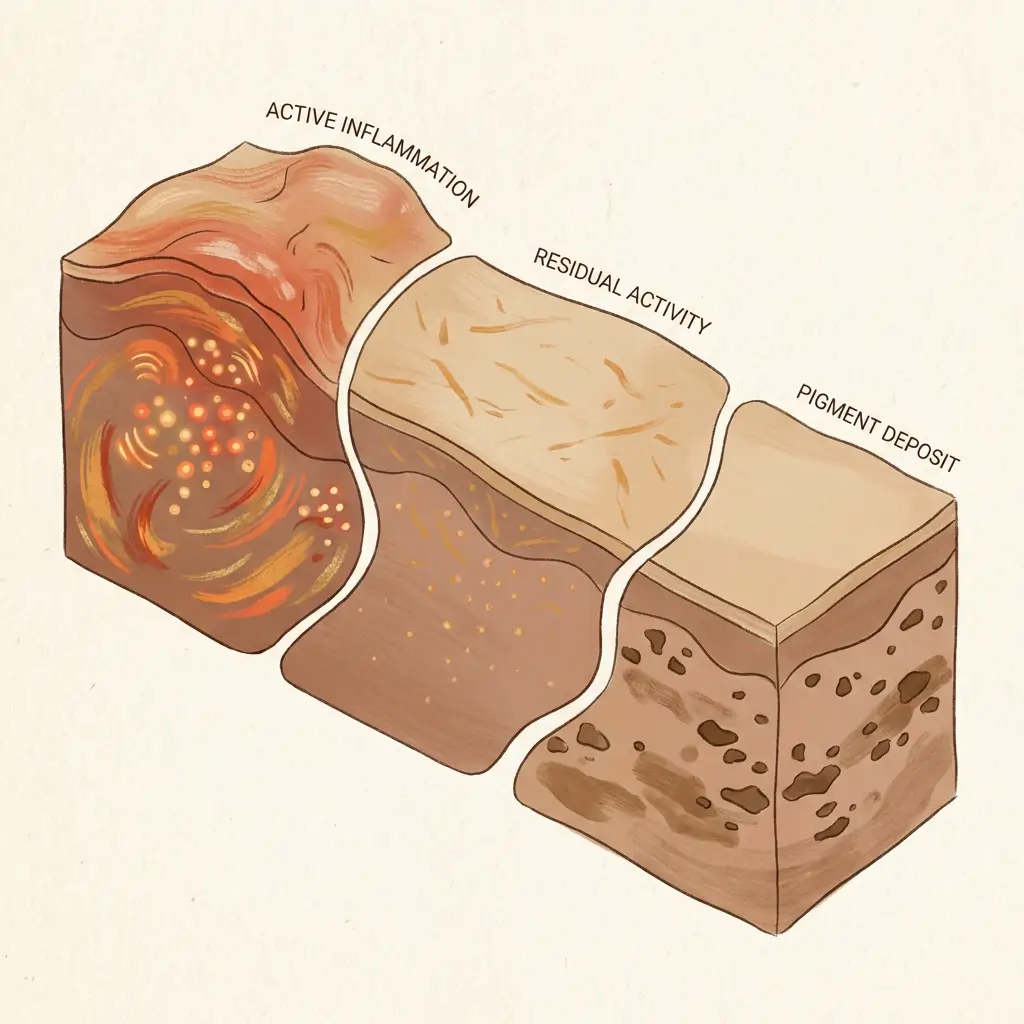
- In intense episodes, melanin gets pushed deeper into the dermis, below the reach of normal skin turnover entirely
That last point is key. The cells responsible for clearing dermal melanin (macrophages) work slowly. Months slowly. Sometimes years slowly. They are essentially clean-up crews working one grain at a time on a job that requires heavy machinery.
This is also why two people can get the same type of mark and have completely different fading timelines. It is not about effort or product quality. It is about where the melanin ended up. Epidermal pigment (upper layers) turns over with your skin cycle. Dermal pigment (deeper layers) requires a biological removal process that operates on its own schedule, regardless of what you apply on the surface.
The sunburn healed weeks ago, but the dark patch is still there. The acne cleared months ago, but the shadow remains. The trigger was temporary. The inflammatory environment it created was not.
That mark you keep waiting on? It is not being lazy. It is literally deeper than your skin's standard recycling system can reach.
Why melanin-rich skin responds more intensely
Everything above happens in all skin. But the volume is not equal.
If you have darker skin, your melanocytes are not just more active at baseline. They are more responsive. They produce melanin faster, in larger quantities, and across a wider range of triggers. This is not a flaw. It is your skin doing exactly what it evolved to do, just at a higher volume.
In practical terms: the same inflammatory event that leaves a faint pink mark on lighter skin can leave a deep brown mark on darker skin. Same biology. Different intensity.
This has real consequences for treatment decisions. Approaches that create their own inflammatory response (certain chemical peels, aggressive retinoid protocols, laser procedures) carry a higher risk of making pigmentation worse in melanin-rich skin. The treatment triggers the very pathway it was trying to interrupt. And that is not a rare side effect. It is a predictable outcome when you apply an inflammatory intervention to skin that is primed to respond to inflammation with pigment.
Many women with deeper skin tones recognise this instinctively, even without the biological explanation:
- A small scratch darkens
- A pimple leaves a mark that lasts months
- An allergic reaction leaves a shadow long after the rash clears
That is not your skin overreacting. It is a proportionally stronger version of this exact pathway. Your skin is not broken. The mechanism is not a mystery. The frustration is real, but the biology is functioning exactly as designed.
Every trigger, same destination
It helps to see just how many different triggers funnel into this one mechanism.
UV exposure damages skin cells directly. The damaged cells release inflammatory cytokines. Melanocytes respond by ramping up melanin. This is technically the tanning response, but when it is excessive, uneven, or happens in skin that is already primed, it tips over into hyperpigmentation. Sunscreen helps limit the initial trigger, but it does nothing about inflammation that is already underway from other sources.
Heat activates inflammatory pathways even without UV. Cooking over a stove, a laptop on your legs, sitting near a radiator, living in a hot climate. No sunburn, no redness, nothing you would identify as a "trigger." Just low-grade thermal stress producing chronic pigment production over time
Acne involves a localised immune response to bacterial infection and follicular rupture. The inflammatory response at the breakout site activates melanocytes in the surrounding tissue. The acne heals. The pigment production stays. This is post-inflammatory hyperpigmentation in its most classic form, and it is the reason a single breakout can leave a mark that takes longer to fade than the blemish took to form.
Friction and pressure create mechanical stress on skin cells, which trips the same inflammatory signalling. Bra straps, waistbands, repeated rubbing. The darkening is not from the rubbing itself. It is from the chronic, low-level inflammatory response the rubbing generates.
Procedures like lasers, microneedling, and chemical peels deliberately create controlled injury. The healing process is inherently inflammatory. Managed well, the result is renewal. Managed poorly, or in skin with a stronger inflammatory response, the result is post-procedure pigmentation.
Internal stressors like hormonal shifts, blood sugar instability, gut dysfunction, and chronic psychological stress generate systemic inflammation that reaches the skin through the bloodstream. Nothing touched your skin. No new products. No sun exposure. But something shifted internally, and the inflammatory signalling found your melanocytes anyway. These are the hardest drivers to identify because there is no visible trigger to point to.
Different stories. Same ending. Same pathway.
What this changes about how you approach treatment
This is not a treatment article, so no protocols here. But understanding the common pathway rewires the logic.
If inflammation is the shared mechanism, then calming inflammation is not one step in a plan. It is the foundation. Before you choose a serum, before you book a procedure, before you start a retinoid, the real question is: what is the inflammatory state of your skin right now, and what is driving it?
Think about what happens when you skip that question:
- You layer actives onto skin that is already inflamed. You feed the cycle.
- You undergo a procedure while systemic inflammation is high. You get rebound pigmentation.
- You treat the surface mark without addressing the internal driver. The mark fades. A new one appears.
Sound familiar?
This is why women who have tried multiple products and seen limited results are not failing at skincare. They are often treating the visible pigment without addressing the invisible process that created it. The treatment approaches that produce lasting change tend to be the ones that account for this.
Calming inflammation means sequencing correctly. Choosing ingredients that reduce inflammatory signalling rather than adding to it. Recognising that what is happening beneath the skin matters at least as much as what you put on top.
It also means being honest about the internal piece. If your inflammation is being driven by something systemic (hormones, stress, blood sugar, gut health), then no topical in the world is going to fully resolve the pigment it produces. You can fade marks on the surface while the system underneath keeps generating new ones. That is not a skincare failure. That is an incomplete strategy.
For some women, this shift in thinking is the thing that finally breaks the cycle. Not a new product. Not a new procedure. Just a clearer understanding of what was actually driving the pigment all along.

Every trigger has its own story. But they all speak the same language. Learn that language, and you stop chasing symptoms and start addressing the process.


