


You went in for a laser treatment or a peel to fix your dark spots. The clinic told you it was safe. You followed the aftercare. And a few weeks later, the spots came back darker than before.
If that has happened to you, or if you are trying to make sure it does not, this explains why it happens. Not in vague terms. The actual biology, so you can see where the risk sits and make better decisions about whether, when, and how to pursue procedures.
The catch-22 at the centre of every procedure
Every cosmetic procedure that improves skin does it by injuring skin first. That is the entire premise. A laser burns a controlled layer off. A chemical peel dissolves it. Microneedling punctures it thousands of times. Then your body heals, and the new skin that forms is (ideally) smoother and more even.
The problem is in the healing part.
When your body repairs damaged tissue, it sends out a rush of inflammatory signals. Think of it like an alarm system going off. Immune cells arrive, swelling kicks in, and a wave of chemical messengers start coordinating the rebuild. That inflammatory response is what makes the healing happen. Without it, nothing gets repaired.
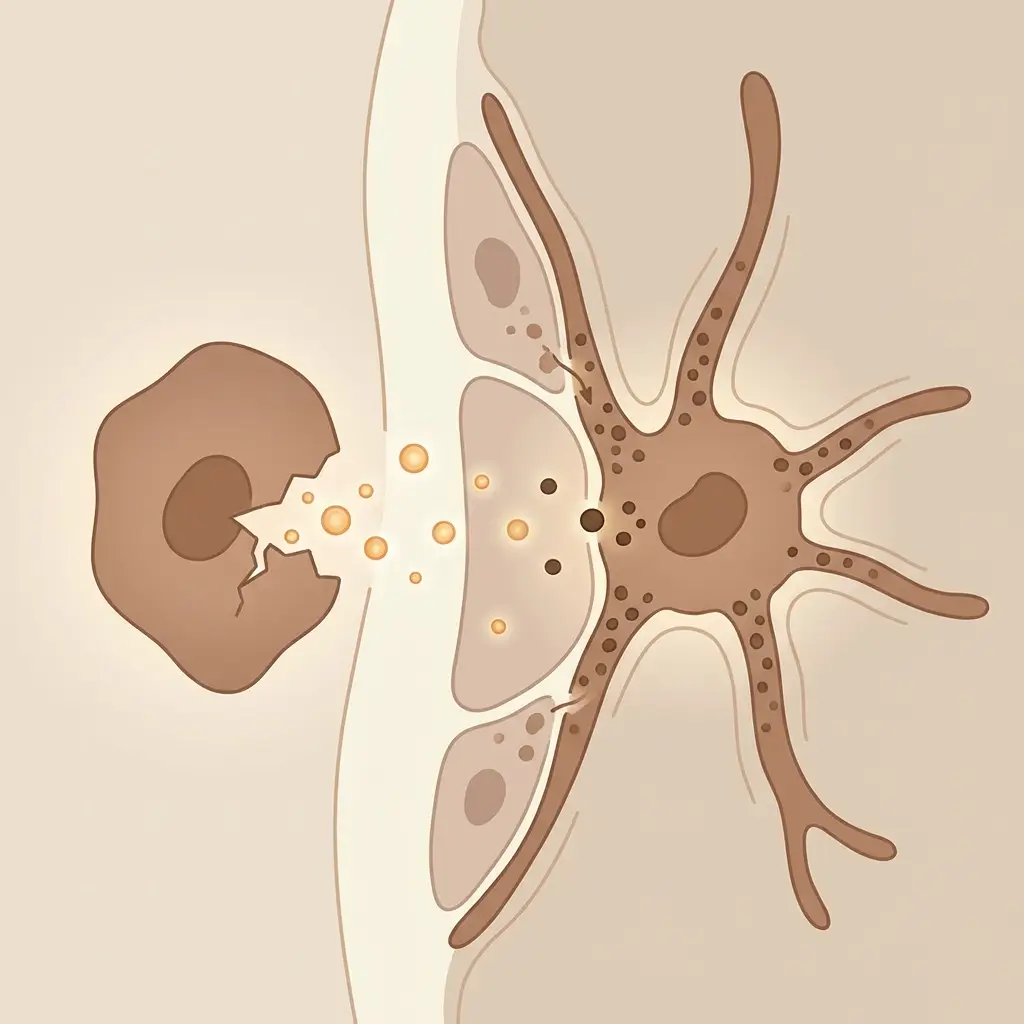
But here is what most clinics do not explain clearly enough: some of those same chemical messengers also talk directly to your melanocytes, the cells that produce pigment. When melanocytes pick up those signals, they interpret them as a threat. And their response to a threat is always the same. Make more melanin. Push it out into the surrounding skin. Darken the area.
Your skin is not broken when this happens. It is actually trying to protect you. Melanin acts like a shield over damaged tissue, guarding it from UV while it is vulnerable. That is a genuinely useful response if you have a wound. It is a terrible response if you just paid to have pigmentation removed.
This is the catch-22. The healing process that makes procedures work runs through the exact same pathway that triggers new pigment.
If you have darker skin, the margin for error is smaller
This is the part that does not get said often enough, and it is the part that matters most if you have melanin-rich skin.
Everyone has roughly the same number of melanocytes, regardless of skin tone. The difference is how active those melanocytes already are at baseline, and how easily they are triggered into overdrive.
If your skin is darker, your melanocytes are already working harder. Their melanin-producing machinery is more efficient. Their melanosomes (the tiny packets that hold and transport pigment) are larger and more evenly spread. All of this is completely normal and healthy. But it also means that the amount of inflammation needed to tip them into overproduction is lower.
A simple way to think about it: imagine two engines, one idling at 1,000 RPM and one at 3,000. Both can redline. But the one already running higher gets there faster, with less input. That is what is happening with melanocytes in darker skin. The threshold between "controlled healing" and "unwanted pigment surge" is narrower.
On top of that, melanin-rich skin also tends to produce a stronger inflammatory response in general. So not only is the trigger threshold lower, the volume of signals hitting the melanocytes is higher and lasts longer.
This does not mean procedures cannot work for darker skin. It means the settings, the approach, and the provider's experience with your skin type matter far more than they would for someone with lighter skin. The same procedure, at the same intensity, can be perfectly fine for one person and cause significant post-inflammatory hyperpigmentation in another. The biology is just different.

Different procedures, different levels of risk
Not all procedures create the same amount of inflammation, and that really matters for pigment risk.
- Ablative lasers (CO2, erbium) are the most aggressive. They vapourise layers of skin and create deep thermal damage. The inflammatory response is intense and the healing window is long. For darker skin, the pigment risk is high enough that many experienced providers avoid these entirely, or only use them in fractional mode at conservative settings.
- Non-ablative lasers (like Nd:YAG at 1064nm) heat the deeper layers without destroying the surface. The pigment risk is meaningfully lower, but it is not zero. Pushed too hard or without enough cooling, they can still cross the threshold.
- Chemical peels vary enormously depending on the acid, the strength, and how long it stays on. A light mandelic peel is a very different animal to a medium-depth TCA peel. And the same percentage of the same acid can behave differently depending on your prep regimen and your skin's condition that day.
- Microneedling spreads its damage across thousands of tiny punctures rather than concentrating it, which generally makes it lower risk. But depth, speed, number of passes, and what gets applied to your skin during the procedure all affect how much inflammation builds up. Aggressive microneedling with potent serums pushed into open channels can still provoke a pigment response.
The point is not that one type is safe and another is dangerous. It is that every procedure sits on a spectrum, and the inflammatory dose it delivers is what determines the outcome.
Why your provider is the most important part of the equation
You cannot change your biology. What you can change is who you trust with it.
A skilled provider calibrates every parameter of a procedure to stay within your safe range. That looks different depending on the treatment:
- Lasers: fluence, pulse duration, spot size, cooling, number of passes
- Peels: acid type, concentration, contact time, pre-treatment prep
- Microneedling: needle depth, speed, pressure, number of passes
The providers who get consistently good outcomes in melanin-rich skin are not using different machines. They are using the same machines with different settings, because they understand how their patient's skin will respond. That experience is specific. Being excellent with lighter skin does not automatically translate.
A few things worth paying attention to before you book:
- If a provider uses the same protocol for every skin tone, they are not calibrating for you.
- If they push for aggressive settings to get dramatic results in one session, they are prioritising short-term impact over your long-term safety.
- If they do not bring up the specific risk of post-inflammatory hyperpigmentation before performing a procedure on your skin, they have not done adequate informed consent.
None of this means procedures are off the table. It means the person holding the device matters as much as the device itself.
What happens after you leave matters just as much
There is a tendency to think of the procedure as the main event and everything after as basic aftercare. In reality, it is closer to the opposite.
The procedure takes minutes. The inflammatory environment it creates can last weeks. During that entire window, your melanocytes are sensitised and primed to overreact to things they would normally handle fine.
- Sun exposure during the healing window hits melanocytes that are already on high alert. This is the single fastest way to trigger new pigment after a procedure.
- Irritating actives (retinoids, strong acids, vitamin C at high concentrations) introduced too soon can extend or reopen the inflammatory window.
- Heat from saunas, intense workouts, or even just hot weather can sustain low-grade inflammation long after the visible redness has faded.
What happens after you leave the clinic is not a footnote. It is half the procedure.

What to take from this
Understanding this mechanism is not about scaring yourself away from procedures. It is about seeing clearly what is actually happening beneath the surface, so your decisions about provider, device, settings, timing, and aftercare are based on biology rather than marketing copy.
The inflammation-to-pigment pathway is not a flaw in your skin. It is one of its oldest defence systems. Procedures that work through controlled injury are working with that system, and the question is never whether inflammation will occur. It always will. The question is whether the people involved, you and your provider, understand the threshold you are working within.
That understanding is what separates a procedure that helps from one that sets you back.


